
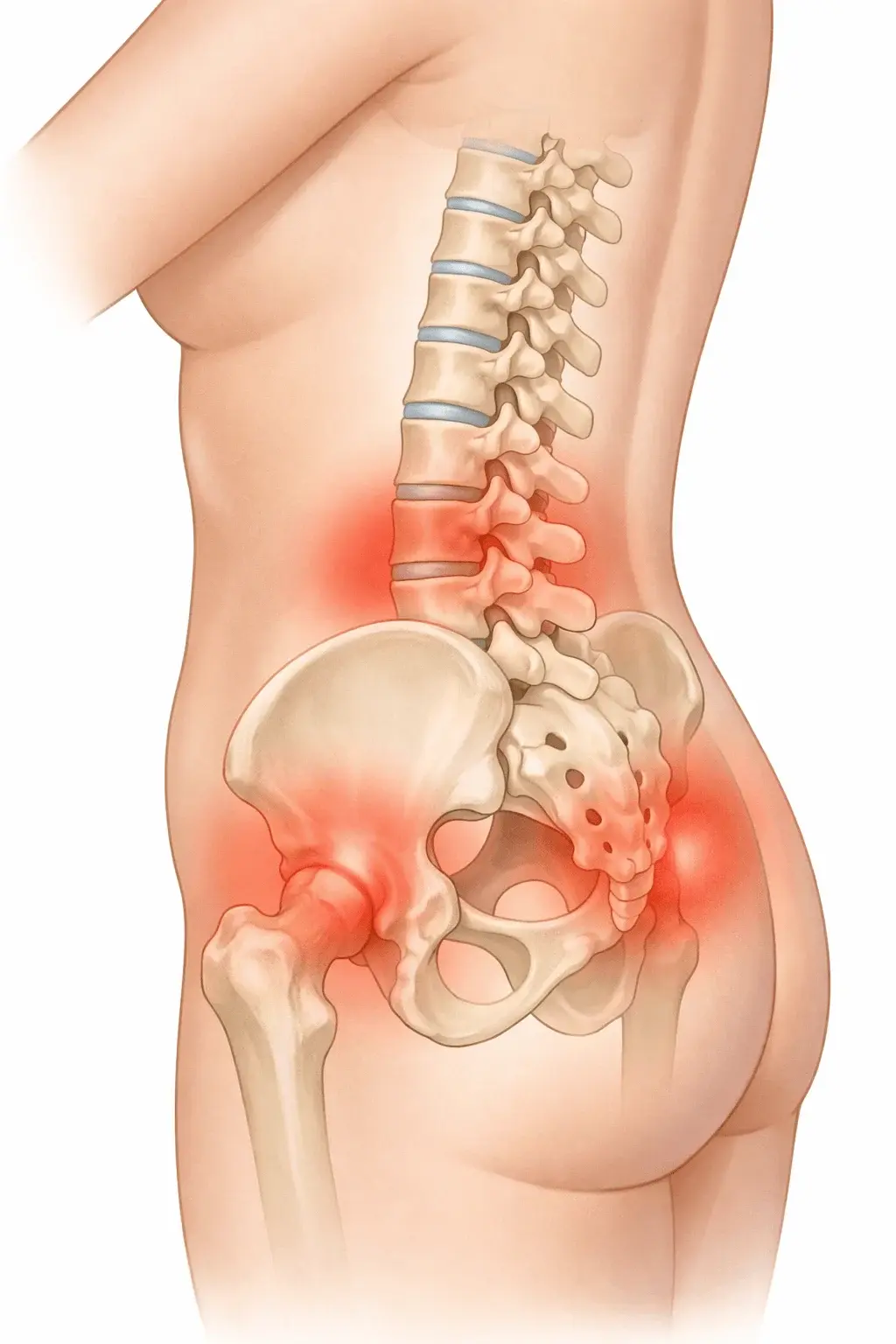
Why Menopause Triggers Back and Hip Pain
The connection between menopause and lower back pain isn't just coincidence. Estrogen receptors exist throughout your musculoskeletal system, including spinal discs, tendons, and hip joints. When estrogen declines during perimenopause and menopause, these tissues lose critical support for maintaining hydration, elasticity, and inflammation control. What many women experience as sore hips menopause or perimenopause backache often reflects this systemic shift rather than isolated injury.
Here's what actually happens: declining estrogen reduces collagen production in connective tissues, making tendons and ligaments less resilient. Simultaneously, bone density decreases, altering spinal alignment and joint stability. The result is menopausal tendonitis and inflammation that manifests as persistent aching, morning stiffness, or sharp pain during movement. Women who previously managed occasional discomfort often report extreme lower back pain menopause that disrupts sleep and daily activities.
The pattern differs from mechanical back pain. Rather than worsening with specific movements, hormonal pain tends to be more diffuse, affecting both lower back and hip pain menopause simultaneously. Some women notice their pain correlates with hot flashes and lower back pain occurring together, as both stem from hormonal fluctuations. Managing stress during menopause becomes crucial, since cortisol amplifies inflammatory responses that worsen joint pain.
Understanding whether you're experiencing perimenopause and back pain versus postmenopausal back pain matters for treatment timing. During perimenopause, hormones fluctuate wildly, causing pain that comes and goes unpredictably. Post-menopause, estrogen remains consistently low, leading to steadier but often more persistent discomfort. Women in early perimenopause who address low estrogen and hip pain proactively tend to experience less severe symptoms later.
What Actually Helps vs. Common Myths
Myth: Rest is the best treatment. While acute pain may require brief rest, prolonged inactivity actually worsens postmenopausal back pain by allowing muscles to weaken and joints to stiffen. Evidence shows that gentle, consistent movement—particularly weight-bearing exercise—stimulates bone maintenance and improves joint lubrication. The key is finding the threshold between helpful movement and overexertion.
Myth: Pain means damage. Many women avoid activities when experiencing perimenopause and hip pain, fearing they're causing harm. However, hormonal pain often exists without structural injury. The discomfort reflects inflammatory changes and tissue adaptation rather than tissue destruction. This distinction matters because movement-based treatments remain safe and effective even when pain is present.
Evidence-Based Relief Strategies
- Resistance training 2-3x weekly: Builds muscle support around vulnerable joints and stimulates bone density through mechanical loading
- Anti-inflammatory nutrition: Omega-3 fatty acids, vitamin D supplementation (often deficient in women with joint pain), and reduced processed foods
- Hormone replacement therapy (HRT): Studies show systemic estrogen can reduce musculoskeletal pain when started during perimenopause, though benefits diminish if initiated years after menopause
- Physical therapy for menopausal tendonitis: Eccentric strengthening exercises specifically target tendon resilience, offering more benefit than passive treatments like massage alone
One overlooked factor: sleep quality directly impacts pain perception. Women experiencing both back pain and hot flashes often find that treating night sweats improves daytime pain tolerance. Similarly, addressing PMS during perimenopause can prevent cyclical pain flares that compound baseline discomfort.
For menopause hip pain relief, targeted hip strengthening exercises prove more effective than general stretching. Focus on gluteal activation and hip external rotation exercises, which stabilize the joint and reduce compensatory stress on the lower back. Many women find relief within 4-6 weeks of consistent practice, though improvement can be gradual rather than immediate.

When Standard Advice Doesn't Work
Not every case of can menopause cause back pain follows the typical pattern. Some women experience worsening symptoms despite implementing all recommended strategies. This often signals an underlying condition that coincides with menopause but requires separate treatment. Conditions like facet joint arthritis, spinal stenosis, or sacroiliac joint dysfunction can intensify during hormonal transition, creating a complex pain picture that doesn't respond to hormone therapy alone.
Women with pre-existing autoimmune conditions face particular challenges. Rheumatoid arthritis and lupus frequently flare during perimenopause, making it difficult to distinguish between can menopause cause hip and leg pain versus disease progression. In these cases, coordinating care between rheumatology and gynecology becomes essential. Standard menopausal tendonitis treatment may need modification to account for immunosuppressive medications or higher baseline inflammation.
Another scenario where typical advice fails: women who cannot take HRT due to contraindications. For them, the question of how to treat menopause back pain requires alternative approaches like selective estrogen receptor modulators, targeted physical therapy protocols, and aggressive lifestyle modification. These women often need more frequent monitoring and adjustment of their treatment plans, as the absence of hormonal support means relying entirely on mechanical and inflammatory management strategies.
If you've tried multiple approaches without improvement over 3-4 months, consider imaging studies to rule out structural issues. While most backache and menopause cases resolve with conservative treatment, persistent pain warrants investigation. This isn't admitting defeat—it's ensuring you're treating the right problem with the right tools.
