
Understanding Menopausal Vaginal Dryness: Why Regular Lubricants Often Fail
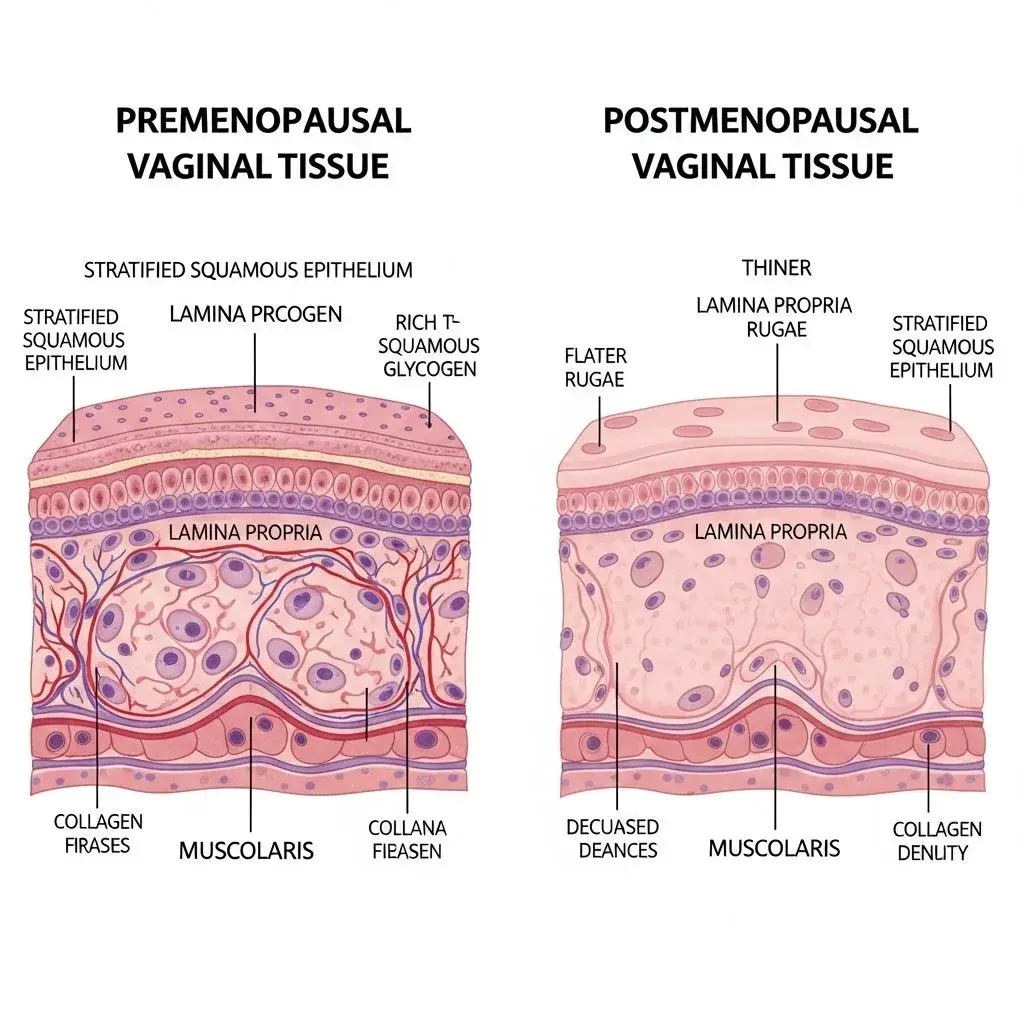
Menopausal vaginal dryness isn't simply reduced lubrication—it's a fundamental change in tissue structure called vaginal atrophy or genitourinary syndrome of menopause. Estrogen decline causes vaginal tissue to thin, lose elasticity, and produce drastically less natural moisture. The pH shifts from acidic (3.8-4.5) to nearly neutral (5.0-7.0), disrupting the protective bacterial environment. This explains why lubricants designed for premenopausal women often cause burning, irritation, or don't provide adequate relief—they're solving the wrong problem.
The tissue changes create a specific set of requirements that standard lubricants ignore. Thinned vaginal walls are more susceptible to micro-tears, meaning you need formulas that provide long-lasting slip without friction. The altered pH makes you vulnerable to infections, requiring pH-balanced products rather than generic options. Many women report that lubricants they used successfully for decades suddenly cause stinging or dryness rebound—this isn't product failure, it's incompatibility with transformed tissue. Understanding vaginal health changes is essential, as explored in our guide to bacterial vaginosis and yeast infections during menopause.
Additionally, absorption rates change dramatically. Menopausal vaginal tissue absorbs ingredients differently than young tissue, meaning certain lubricant bases that once stayed on the surface now penetrate and cause irritation. This physiological shift demands reformulating your approach—what worked at 40 may be actively harmful at 55, not due to product quality but tissue compatibility.
Common Myths vs. What Evidence Shows Works
Myth: Water-Based Lubricants Are Always the Safest Choice
Water-based lubricants dominate recommendations because they're condom-compatible and easy to clean, but for menopausal women they often provide inadequate relief. These formulas evaporate quickly on already-dry tissue, requiring frequent reapplication that disrupts intimacy. Many contain glycerin or propylene glycol as humectants—these ingredients can cause osmotic imbalance in menopausal tissue, actually drawing moisture out of cells and causing burning sensations or yeast infections.
What works better: hyaluronic acid-based water formulas specifically designed for vaginal atrophy, or switching to silicone-based lubricants. Hyaluronic acid binds water more effectively and doesn't disrupt osmolality. Silicone lubricants last significantly longer—sometimes 4-6 times longer than water-based—meaning one application suffices where water-based requires multiple interruptions. The trade-off is cleanup: silicone requires soap and water, while water-based washes away easily. For menopausal women prioritizing effectiveness over convenience, this trade-off usually favors silicone.
Myth: You Only Need Lubricant During Sexual Activity
The distinction between lubricants (for sexual activity) and vaginal moisturizers (for daily tissue health) confuses many women, causing them to address only immediate friction rather than underlying atrophy. Vaginal moisturizers are leave-in products used 2-3 times weekly that hydrate tissue continuously, improving baseline moisture levels. Lubricants provide temporary slip during activity but don't treat the chronic dryness.
Most menopausal women need both: daily or regular moisturizers to maintain tissue health, plus lubricants during intimacy for additional slip. Using only lubricants means you're constantly fighting severe baseline dryness, while moisturizer alone may not provide enough glide during friction activities. This two-product approach contradicts the simpler single-product routine most women expect, but it reflects the reality that menopausal vaginal changes require maintenance beyond point-of-use solutions.
Choosing the Right Lubricant: Matching Formula to Your Specific Situation
For Mild to Moderate Dryness: pH-Balanced Hyaluronic Acid Formulas
If you experience occasional dryness or discomfort but still produce some natural lubrication, hyaluronic acid water-based lubricants designed for menopausal women offer the best balance. Look for products specifically labeled pH 4.5 or vaginal pH-matched and free from glycerin, parabens, and warming/tingling agents. These formulas support your natural pH while providing temporary moisture boost without irritation.
Application matters: use these 10-15 minutes before activity to allow absorption, which creates better glide than last-second application. For women still using condoms, this category is essential since silicone and oil-based options may degrade latex. The limitation: these don't last as long as silicone, so longer intimate sessions may require reapplication. Some women keep a small amount beside the bed for discreet mid-activity refreshing.
For Severe Dryness or Painful Intercourse: Medical-Grade Silicone
When dryness causes pain, bleeding, or makes intimacy impossible, medical-grade silicone lubricants provide superior long-lasting slip that doesn't evaporate or absorb into tissue. A small amount (pea-sized) typically suffices for entire encounters, whereas water-based formulas might require tablespoon quantities. Silicone creates a genuine moisture barrier that protects fragile tissue from friction damage.
The downside: silicone stains fabric and requires thorough cleanup with soap. It's incompatible with silicone toys, which limits some activities. However, for women experiencing dyspareunia (painful intercourse), the superior protection often outweighs these inconveniences. Many gynecologists specifically recommend silicone for severe vaginal atrophy cases. Combine with regular vaginal moisturizer use—silicone handles immediate friction needs while moisturizers address chronic tissue health. This comprehensive approach is similar to strategies discussed in Davina McCall's menopause supplement approach—addressing symptoms from multiple angles simultaneously.
When Standard Options Fail: The Hormone Therapy Conversation
There's a threshold where no lubricant adequately compensates for severe vaginal atrophy. If you're using substantial amounts of lubricant, still experiencing pain, seeing spotting after intimacy, or avoiding sexual activity entirely due to discomfort, lubricants alone aren't solving your problem. This represents the honest limitation of over-the-counter solutions—they manage symptoms but don't reverse the underlying tissue deterioration.
At this stage, discuss vaginal estrogen therapy with your healthcare provider. Local estrogen (creams, tablets, or rings applied directly to vaginal tissue) can reverse atrophy by restoring tissue thickness, elasticity, and natural moisture production. This isn't admitting defeat—it's recognizing when physiology requires medical intervention beyond topical products. Many women use both vaginal estrogen for tissue restoration and lubricants for additional comfort, finding this combination finally provides the relief that lubricants alone couldn't achieve.
