
Why Menopause Triggers Burning Skin Sensation
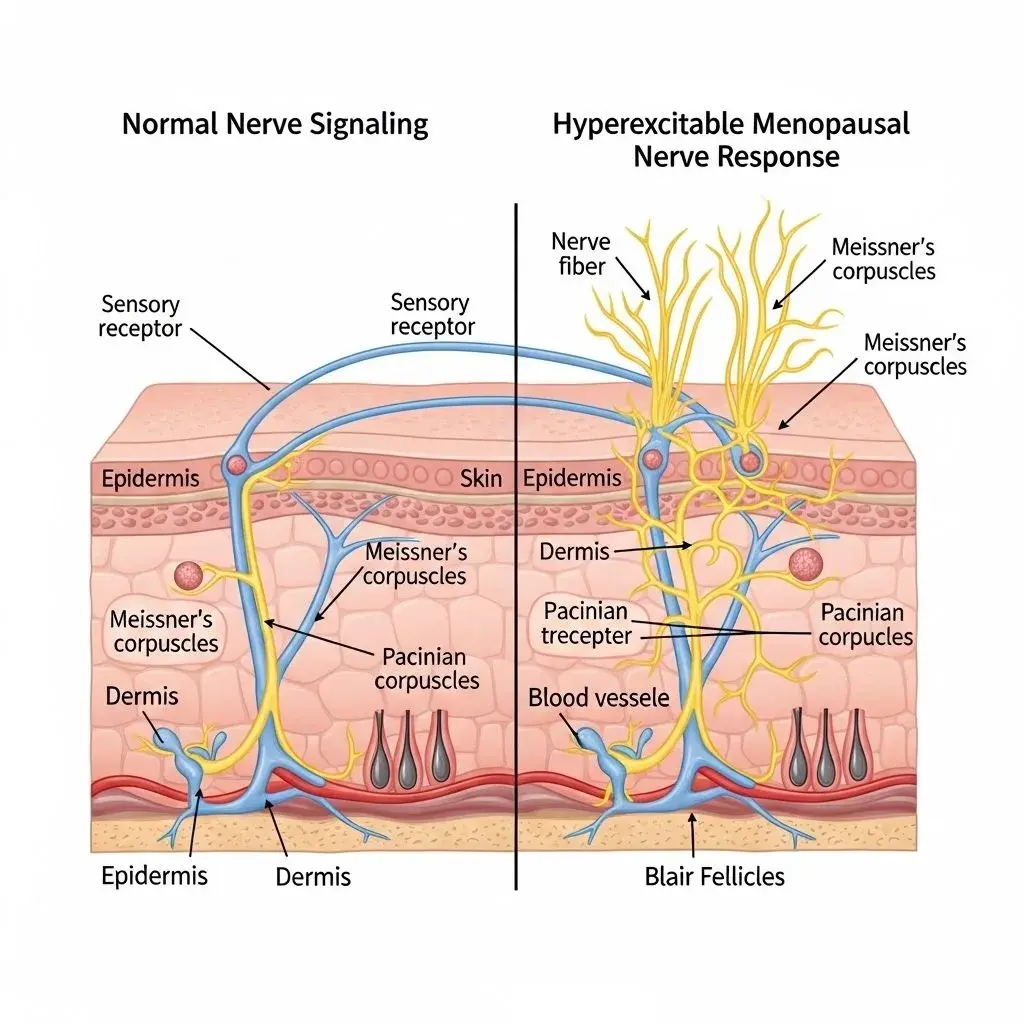
The phenomenon of menopause and burning skin sensation isn't psychological or imagined—it's a documented neurological response to declining estrogen levels. Estrogen receptors exist throughout your peripheral nervous system, particularly in the small nerve fibers responsible for temperature and pain sensation. When estrogen drops during perimenopause and menopause, these nerve fibers become hyperexcitable, sending pain signals in response to stimuli that previously caused no discomfort. This explains why your skin might feel like it's burning when touched by clothing, sunlight, or even air movement.
Research shows that approximately 20-25% of menopausal women experience some form of abnormal skin sensation, technically called paresthesia. The burning variant often manifests as prickly heat menopause—a crawling, tingling, or burning feeling that moves across the skin surface without visible cause. This differs from hot flashes, though they often occur together. While hot flashes involve vasomotor temperature dysregulation, burning skin sensation stems from nerve fiber dysfunction. The dual mechanism explains why cooling strategies that work for hot flashes sometimes fail to relieve the burning sensation.
The critical factor most women don't realize: skin barrier disruption amplifies nerve sensitivity. Declining estrogen reduces ceramide production and natural moisturizing factors, thinning the protective barrier that normally shields nerve endings from external irritants. When this barrier weakens, everything from synthetic fabrics to skincare preservatives can trigger exaggerated nerve responses. This creates a feedback loop where barrier damage increases sensitivity, and heightened sensitivity causes behaviors like scratching that further damage the barrier. For comprehensive barrier repair strategies, see our guide to skincare for hormonal changes.
Common Misconceptions About Burning Skin During Menopause
Myth 1: It's Just Anxiety or Stress
The dismissive attitude that burning skin sensation is psychosomatic contradicts neurological evidence. While anxiety can lower pain thresholds, the burning sensation originates from measurable changes in nerve fiber density and function. Skin biopsies of menopausal women show reduced small fiber nerve density compared to premenopausal controls. This is a physical change, not an emotional manifestation. The frustration comes when healthcare providers suggest the problem is stress-related without investigating the hormonal neurological connection.
Myth 2: Cooling Products Solve the Problem
What beginners misunderstand about prickly heat menopause relief: menthol and cooling ingredients provide temporary distraction through counter-irritation, but they don't address nerve hyperexcitability. In fact, menthol can sometimes worsen symptoms by further stimulating already-overactive nerve receptors. The trade-off is immediate relief for 15-30 minutes followed by potential rebound sensitivity. More effective long-term strategies focus on nerve stabilization through ingredients like palmitoylethanolamide (PEA) or barrier repair with ceramides.
Myth 3: The Sensation Always Indicates Skin Damage
Here's the contradiction that confuses most women: your skin can feel intensely burned without any visible redness, rash, or damage. This disconnect between sensation and appearance happens because the problem lies in nerve signaling, not tissue injury. The nerves are sending pain signals without proportional cause. However, this doesn't mean you should ignore the sensation—chronic nerve pain can lead to actual inflammation and barrier damage through stress pathways and behavioral responses like rubbing or over-washing.
Evidence-Based Relief Strategies That Work
The most effective approach to burning skin sensation combines nerve stabilization, barrier repair, and trigger avoidance. These work synergistically rather than in isolation—stabilizing nerves reduces reactivity, barrier repair protects nerve endings, and avoiding triggers prevents flare cycles. What experienced practitioners prioritize first is identifying your personal trigger pattern, which varies significantly between individuals.
Immediate relief strategies that address nerve hypersensitivity:
- Colloidal oatmeal baths (lukewarm, not hot): The avenanthramides in oatmeal reduce nerve-mediated inflammation and create a protective film over nerve endings. Soak for 15-20 minutes, pat dry gently, and apply barrier repair immediately while skin is damp.
- Ceramide-rich moisturizers applied within 3 minutes of water exposure: This timing is critical—damp skin absorbs ceramides more effectively, and the occlusive layer prevents trans-epidermal water loss that exacerbates nerve sensitivity.
- Natural fiber clothing (cotton, bamboo, silk): Synthetic fabrics create friction and static electricity that trigger hyperexcitable nerves. Wash new clothes 2-3 times before wearing to remove manufacturing chemicals that irritate compromised barriers.
Long-term management requires addressing the hormonal root cause. Systemic hormone replacement therapy (HRT) can normalize nerve function in 60-70% of women experiencing burning sensations, though effects take 8-12 weeks to manifest. For those who cannot or choose not to use HRT, topical estrogen applied to affected areas may provide localized nerve stabilization without systemic exposure. Supplements like evening primrose oil (1-3g daily) or black cohosh show modest efficacy in some studies, though evidence remains mixed. Related symptoms like itchy ears during menopause often respond to similar nerve-stabilizing approaches.
When Standard Relief Methods Fail
Here's the edge case that derails typical recommendations: some women develop burning skin sensation not from estrogen decline alone, but from thyroid dysfunction that commonly emerges during menopause. Hypothyroidism causes peripheral neuropathy with identical burning symptoms, but thyroid-related nerve pain doesn't respond to barrier repair or standard menopause interventions. If your burning sensation worsens despite addressing hormonal and barrier factors, or if you also experience unexplained fatigue, cold intolerance, or cognitive changes, request thyroid function testing including TSH, free T3, and free T4. The limitation is that standard menopause treatment protocols don't screen for this overlap, meaning many women spend months trying ineffective barrier repair when they need thyroid medication. Conversely, some providers jump to thyroid diagnosis without addressing the menopause component, when both issues require simultaneous treatment.

