
Why Your Regular Face Cream Stops Working During Menopause
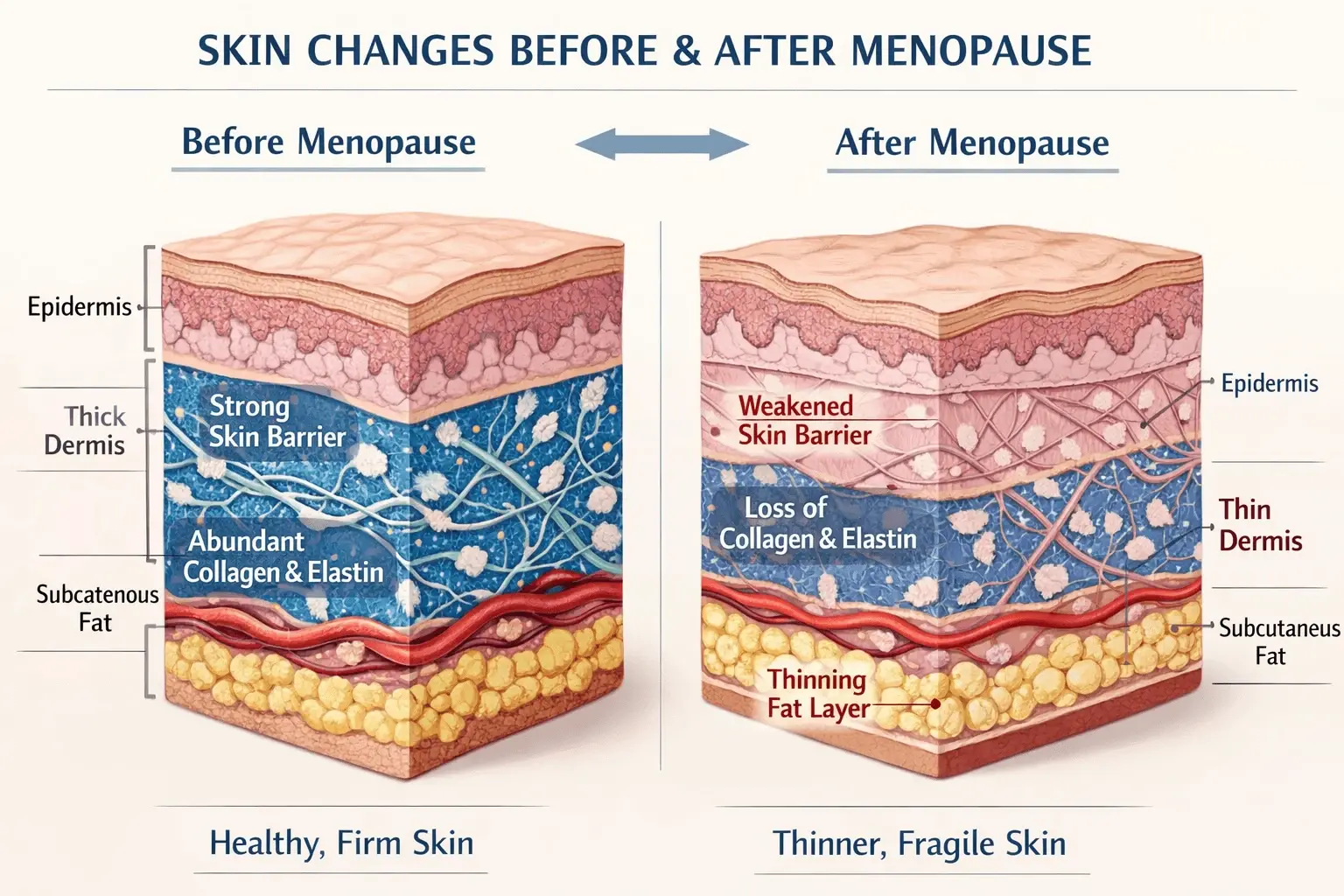
The menopause face cream you need differs fundamentally from regular anti-aging products because declining estrogen triggers cascading skin changes that standard formulas weren't engineered to address. Estrogen receptors throughout your skin regulate everything from collagen production to moisture retention to barrier integrity—when estrogen levels plummet during menopause, these functions collapse simultaneously rather than gradually declining. Your skin loses approximately 30% of its collagen in the first five years post-menopause, experiences dramatic thinning of the dermis, develops compromised barrier function causing increased trans-epidermal water loss, and shifts toward inflammatory responses. The moisturizer that worked beautifully at 45 fails at 52 not because the formula changed but because your skin's fundamental biology transformed.
Here's what dermatologists understand about menopause skin care that beauty marketing rarely explains: the visible changes—dryness, sagging, thinning, texture irregularities—stem from specific hormonal mechanisms requiring targeted intervention rather than generic anti-aging approaches. Declining estrogen directly reduces fibroblast activity that produces collagen and elastin. It decreases hyaluronic acid synthesis in the dermis, causing volume loss and dehydration. It compromises sebaceous gland function, creating dryness even in women who had oily skin their entire lives. Most importantly, it weakens the skin barrier's lipid matrix, making skin simultaneously dry and reactive. Effective menopausal skincare must address these specific mechanisms, not just provide rich moisture or generic peptides.
The critical factor most advice overlooks: skincare for menopausal skin requires layering multiple targeted products rather than expecting one miracle cream to solve everything. Your skin needs barrier repair through ceramides and cholesterol, moisture retention through multiple molecular weights of hyaluronic acid, collagen stimulation through retinoids or peptides, antioxidant protection against increased oxidative stress, and often phytoestrogens to partially compensate for hormonal loss. No single product contains all these elements in effective concentrations—you need a strategic routine addressing each mechanism individually. The failure of menopausal women to see results often comes from using one product when five are needed.
The Phytoestrogen Controversy Nobody Explains Honestly
Phytoestrogens—plant compounds that weakly bind to estrogen receptors in skin—appear in many menopause-targeted face creams as soy isoflavones, red clover extract, or flax lignans. These ingredients theoretically compensate for declining estrogen by activating the same receptors, potentially stimulating collagen production and improving barrier function. However, their effectiveness remains controversial because topical absorption and receptor activation vary dramatically between individuals, and most studies showing benefits used oral supplementation rather than topical application. Some women experience noticeable improvement in skin thickness and hydration with phytoestrogen-containing creams, while others see no difference from regular moisturizers.
What endocrinologists and dermatologists know about skin cream for menopause with phytoestrogens: they work best as part of comprehensive hormone-aware skincare rather than standalone solutions. Women on hormone replacement therapy typically see better results from traditional anti-aging ingredients than from phytoestrogens because they're already compensating for estrogen loss systemically. Women not on HRT may benefit more from topical phytoestrogens, though results vary. The key is treating phytoestrogens as potentially helpful additions rather than miracle cures, and combining them with proven ingredients like retinoids, niacinamide, and barrier-repair lipids that work through non-hormonal mechanisms.
Which Ingredients Actually Work for Menopausal Skin Changes
Retinoids remain the gold standard for addressing menopausal collagen loss because they directly stimulate fibroblast activity and collagen synthesis regardless of hormonal status. However, menopausal skin often cannot tolerate the retinoid concentrations that worked in your forties due to compromised barrier function and increased sensitivity. Start with gentler retinoid forms like retinyl palmitate or granactive retinoid, or use traditional retinol just once or twice weekly rather than daily. Layer retinoid application over a hydrating serum and under a rich moisturizer to buffer irritation while maintaining efficacy. The goal is consistent use at tolerable strength rather than aggressive treatment causing inflammation that worsens skin quality.
Barrier repair ingredients become non-negotiable for menopause skincare brands specifically because estrogen loss directly compromises the lipid matrix that seals moisture in and irritants out. Look for products containing ceramides, cholesterol, and fatty acids in ratios mimicking natural skin lipids—typically 1:1:1 or 3:1:1 depending on research. These ingredients aren't exciting or trendy but they're essential for restoring barrier function that determines how every other product performs. Without intact barrier, even the most advanced serums penetrate poorly while irritants penetrate excessively, creating a state where nothing works and everything stings.
- Retinoids (retinol, retinyl retinoate): Stimulate collagen production and cell turnover; use gentler forms or lower frequency for compromised barrier
- Ceramides, cholesterol, fatty acids: Repair barrier function essential for retaining moisture and preventing sensitivity
- Multiple weights hyaluronic acid: Attracts and retains moisture at different skin depths; compensates for reduced natural HA
- Niacinamide (vitamin B3): Improves barrier function, reduces inflammation, stimulates ceramide production
- Peptides (especially matrixyl, argireline): Signal collagen production and support structural proteins
- Antioxidants (vitamin C, E, resveratrol): Combat increased oxidative stress from hormonal changes
The layering sequence matters exponentially more on menopausal skin than it did pre-menopause because compromised barrier affects absorption and tolerance. Apply products from thinnest to thickest consistency: essence or hydrating toner first, then serums with active ingredients, then targeted treatments, finally moisturizer to seal everything in. Wait 30-60 seconds between layers to allow absorption rather than immediately piling on products that then sit on the surface or interact negatively. This patient approach maximizes efficacy while minimizing irritation that compromised menopausal skin cannot tolerate.
Texture changes require exfoliation adjustment—not elimination but strategic modification. Menopausal skin still accumulates dead cells causing dullness and rough texture, but aggressive exfoliation damages the already-compromised barrier. Switch from physical scrubs or daily chemical exfoliants to gentle enzymatic exfoliants 1-2 times weekly, or use a low-percentage AHA like lactic acid that provides both exfoliation and hydration. The goal is removing surface buildup without stripping the barrier that took weeks to repair through ceramide-rich products.
For comprehensive understanding of how these skincare changes coordinate with lifestyle factors and medical interventions during menopause, explore our guide on skincare for hormonal changes during menopause that addresses the complete picture of maintaining skin health through this transition.
When Standard Menopause Skincare Advice Completely Fails
The universal recommendation to switch to richer, more emollient creams during menopause fails for the 30-40% of women who develop adult-onset oily skin from hormonal fluctuations affecting sebaceous glands differently. Some women experience the expected dryness, but others find their T-zone becomes oilier while cheeks remain dry, creating combination patterns requiring targeted zoning rather than one rich cream everywhere. Others develop unexpected overall oiliness with concurrent sensitivity, needing lightweight hydrators that don't clog pores rather than heavy creams that cause congestion. The assumption that all menopausal skin is dry leads to inappropriate product recommendations that worsen skin for women with different hormonal responses.
Another scenario where conventional wisdom backfires: women being told to use only gentle, fragrance-free products during menopause because their skin is more sensitive. While many women do develop increased reactivity, some actually become less sensitive as inflammation patterns shift. The blanket recommendation to avoid all actives and use only gentle cleansers and basic moisturizers leaves these women with adequate tolerance languishing in ineffective routines when they could safely use retinoids, acids, and vitamin C that would actually improve their skin. Individual assessment of your specific sensitivity level matters more than following age-based assumptions about tolerance.
The critical contradiction between dermatology research and marketed menopause skincare: products specifically labeled for menopause often contain proprietary blends of plant extracts and peptides that sound impressive but lack the clinical evidence supporting retinoids, niacinamide, and barrier repair lipids. These menopause-specific lines cost premium prices for emotional appeal rather than superior efficacy. Often, a well-formulated routine from regular dermatologist-recommended brands—CeraVe, La Roche-Posay, SkinCeuticals—outperforms expensive menopause-marketed products because the fundamental skin needs are the same; it's the concentrations, combinations, and application frequency that need adjustment for hormonal changes.
What actually fails that nobody discusses: expecting topical skincare alone to fully address dramatic menopausal skin changes without considering systemic hormone replacement therapy. While excellent skincare provides meaningful improvement, it cannot fully compensate for the systemic loss of estrogen affecting skin from the inside. Women on HRT typically achieve better skincare results because they're addressing the root cause while topicals handle surface concerns. Women not on HRT—whether by choice or medical contraindication—need realistic expectations that skincare alone provides partial improvement rather than complete reversal of hormonal aging. This doesn't mean skincare is pointless, but it means understanding its limitations.
The hidden challenge with menopausal skincare: your skin's needs fluctuate during perimenopause as hormone levels swing wildly before stabilizing post-menopause. The routine that worked perfectly last month might cause breakouts or irritation this month because your estrogen levels shifted. This unpredictability frustrates women expecting consistent results from consistent routines. The solution involves having multiple product options—lightweight and rich moisturizers, gentle and active serums—adjusting based on how your skin behaves each cycle rather than following rigid routines. Post-menopause, once hormones stabilize at lower levels, skincare results become more predictable again.
For specific product recommendations and complete routines tailored to different menopausal skin presentations, see our detailed guide to the best skin creams for menopause that includes tested recommendations for dry, combination, and unexpectedly oily menopausal skin types.

